

{kind=link}
Drs. Younger-Jun Ko, Jeong-Ho Yun, Hong-Cheol Yoon, Baek-Il Kim, and Dong-Gained Lee illustrate using a brand new machine to measure biofilm on implants
Introduction
Because the prevalence of dental implant therapies continues to rise, the incidence of peri-implantitis has additionally elevated, posing a big risk to the long-term success of implants.1 Peri-implantitis is characterised by irritation and bone loss attributable to the buildup of biofilm on the implant floor, the place metabolic byproducts produced by pathogenic micro organism set off inflammatory responses and speed up illness development.2
Nevertheless, typical biofilm elimination strategies have proven restricted efficacy, and medical examinations mixed with radiographic imaging are sometimes inadequate for precisely assessing early-stage lesions.3 Specifically, small lesions or delicate biofilm accumulations are troublesome to detect visually, highlighting the necessity for extra exact diagnostic and therapeutic applied sciences.4
To beat these limitations, biofluorescence imaging programs (BIS), resembling quantitative light-induced fluorescence (QLF), have not too long ago gained consideration as revolutionary alternate options.5 QLF makes use of blue seen mild at a selected wavelength (405 nm) to detect purple fluorescence emitted by porphyrins produced by mature bacterial colonies, permitting for the quantitative evaluation of biofilm location and maturity (Determine 1).6 This real-time visualization allows speedy analysis of biofilm elimination from the implant floor, in the end enhancing remedy precision.6,7
In these case experiences, we current a medical instances during which QLF (Qraypen C, AIOBIO, Seoul, South Korea; Determine 2) was used to evaluate biofilm accumulation on the implant floor of a affected person with peri-implantitis and to substantiate biofilm elimination throughout surgical/non-surgical remedy. Moreover, medical parameters resembling probing depth, bleeding on probing, and radiographic bone loss have been evaluated to evaluate remedy outcomes. Moreover, we talk about the constraints of this expertise and its potential for future developments. This case highlights the utility of biofluorescence expertise as an efficient and exact instrument for biofilm detection and elimination within the remedy of peri-implantitis.
Case shows
Sufferers recognized with peri-implantitis reported experiencing persistent discomfort and irritation across the implant website over an prolonged interval. Scientific examination revealed reasonable gingival irritation, bleeding on probing, and pus discharge. Radiographic evaluation confirmed the prognosis by demonstrating vital bone loss across the affected implant.
A biofluorescence imaging system (BIS) was used to establish websites of biofilm accumulation on the implant surfaces previous to the preliminary mechanical debridement. The effectiveness of biofilm elimination was evaluated by re-examining the implant surfaces utilizing BIS, and the disappearance of fluorescence was confirmed.
Scientific parameters together with probing depth, bleeding on probing, and radiographic bone loss have been recorded at baseline and post-treatment to judge the general remedy end result.

Outcomes
Case 1
An 80-year-old feminine affected person visited the Division of Periodontology at Gangnam Severance Dental Hospital, complaining of an odor emanating from the higher proper implant website. As a result of lengthy distance from her residence, she had been unable to attend common check-ups constantly. The affected person had a medical historical past of osteoporosis and had been receiving Denosumab (Prolia®) injections each 6 months for the previous 6 years.
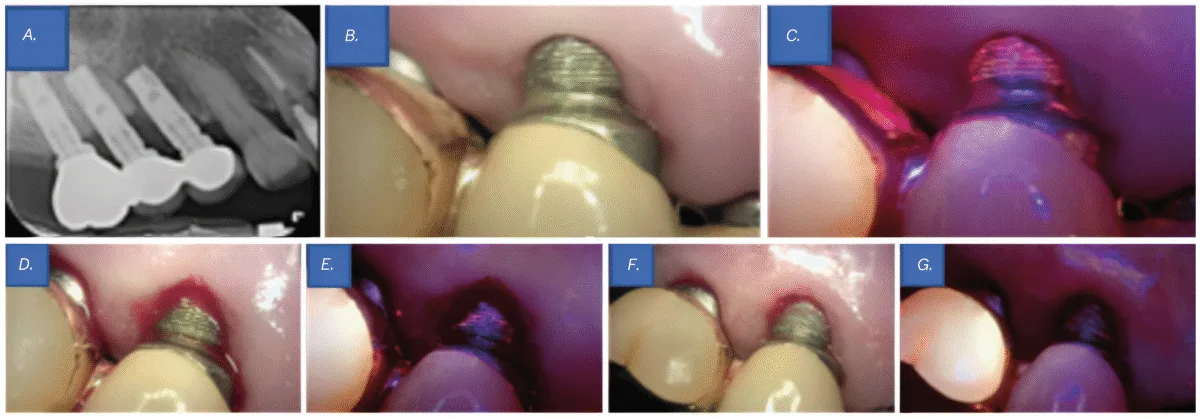
Scientific examination revealed probing depths of 5–6 mm round implant Nos. 4 and 5, with thread publicity at implant No. 5 above the gingival margin. Radiographic examination revealed bone loss round implant Nos. 4 and 5, resulting in a prognosis of peri-implantitis (Determine 3A). Though no vital biofilm accumulation was seen to the bare eye (Determine 3B), analysis utilizing QLF clearly detected biofilm that was not observable beneath typical visible inspection (Determine 3C). Contemplating the affected person’s osteoporosis and the truth that solely 4 months had handed since her final denosumab (Prolia®) injection, flap surgical procedure was not carried out. As a substitute, curettage was chosen because the remedy method.
For biofilm elimination, cleaning was carried out utilizing an ultrasonic scaler (Megagen, Seoul, South Korea), a curette, and a microbrush. After mechanical debridement, QLF imaging was performed once more to match pre- and post-treatment findings. Whereas no biofilm was seen to the bare eye (Determine 3D), QLF revealed residual biofilm on the implant threads (Determine 3E). Extra debridement was carried out, adopted by one other spherical of medical and QLF imaging for affirmation (Figures 3F-3G). This course of enabled a extra thorough analysis of biofilm elimination and served as a visible help for affected person schooling on oral hygiene. Focused brushing instruction (TBI) was additionally offered.
The realm was then rinsed with 0.2% chlorhexidine, and a pair of% minocycline ointment (Periocline®, Sunstar, Osaka, Japan) was topically utilized to the peri-implant lesion for irritation management.
On the 2-week follow-up, peri-implant irritation had considerably decreased, and the affected person reported reduction from discomfort. On the 6-month follow-up, solely delicate irritation was noticed within the surrounding space, however the affected person remained symptom-free, and the peri-implant tissues have been properly maintained.
Case 2
A 70-year-old feminine affected person visited the Division of Periodontology at Gangnam Severance Dental Hospital, reporting bleeding from the decrease left implant website throughout brushing. The affected person had been commonly attending follow-up appointments at our division however had solely obtained non-surgical therapies because of her dental phobia. Medical historical past revealed no vital underlying medical situations.
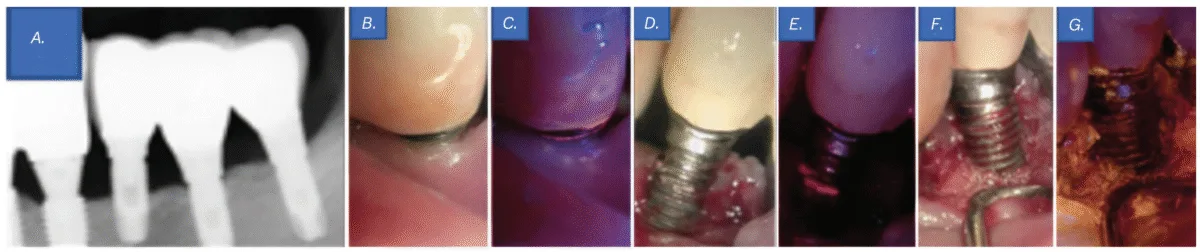
Scientific examination revealed a probing depth of 5–6 mm round implant No. 20, with the implant threads uncovered above the gingiva. Though no vital biofilm attachment was noticed with the bare eye (Determine 4B), QLF revealed the presence of biofilms (Determine 4C). As well as, periapical radiography revealed bone loss round implant No. 20, resulting in a prognosis of peri-implantitis (Determine 4A). Regardless of her dental phobia, the affected person consented to endure flap surgical procedure after an intensive rationalization of the need of actively eradicating components contributing to an infection from the implant floor.
A sulcular incision was constructed from the mesial line angle of No. 21 to the distal line angle of implant No. 19 utilizing #15T and #12 blades. Upon flap elevation, seen biofilm was noticed (Determine 4D), and its presence was confirmed with QLF imaging (Determine 4E). Biofilm elimination was carried out utilizing an ultrasonic scaler (Megagen, Seoul, South Korea), a curette, and a microbrush. Tetracycline was moreover utilized for implant floor decontamination. Subsequent medical and QLF imaging confirmed the profitable elimination of residual biofilm and infectious materials (Determine 4F-4G). The surgical website was then closed utilizing 4-0 absorbable artificial sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, New Jersey) with an interrupted suture method.
One week after the flap surgical procedure, the affected person returned for suture elimination. The therapeutic course of was passable, with no irregular findings. At 6-month and 1-year follow-ups, the affected person reported no discomfort, implant floor hygiene had improved in comparison with the pre-treatment situation, and the general oral well being remained secure.
Case 3
An 86-year-old feminine affected person initially visited a neighborhood dental clinic, the place she was suggested to hunt analysis and remedy at a college hospital because of extreme bone loss across the decrease left implant. She subsequently offered for her first go to to the Division of Periodontology at Gangnam Severance Dental Hospital. The affected person had no vital underlying medical situations apart from hyperlipidemia.
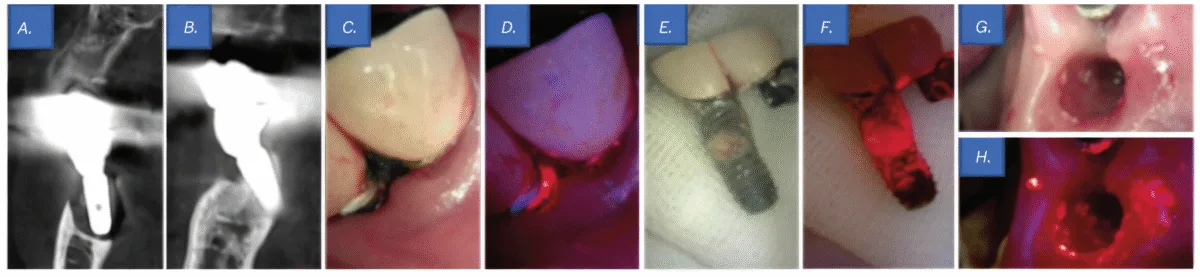
Scientific examination revealed a probing depth of 12 mm round implant No. 19, accompanied by lively pus discharge above the gingival margin (Determine 5C). Moreover, QLF imaging detected purple fluorescence from porphyrins, indicating a mature biofilm (Determine 5D). Cone-beam computed tomography revealed bone loss round implant Nos. 18 and 19, resulting in a prognosis of peri-implantitis (Figures 5A-5B). Notably, implant No. 19 exhibited bone loss extending to the apex, and through prosthesis elimination, it was spontaneously exfoliated (Determine 5E). Though no vital biofilm was noticed macroscopically on the tissue and fixture surfaces (Determine 5G), QLF analysis detected porphyrin fluorescence, confirming the presence of a biofilm (Figures 5F-5H).
Subsequently, a sulcular incision was made utilizing #15T and #12 blades, adopted by socket curettage with tetracycline. The wound was then closed utilizing a figure-eight suture method with 4-0 absorbable artificial sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, New Jersey).
One week after the implant elimination process, the affected person returned for suture elimination. Therapeutic was passable, with no notable issues. On the 6-month follow-up, the affected person reported no vital discomfort, and general oral well being was secure in comparison with the preoperative situation.
Case 4
A 56-year-old male affected person offered for his first go to to the Division of Periodontics at Gangnam Severance Dental Hospital, complaining of frequent meals impaction across the higher left implant space and mobility posterior enamel. Medical historical past revealed no vital underlying medical situations.
Scientific examination revealed a subgingival calculus at website tooth No. 11 and a probing depth of 6 mm at website implant No. 12. Moreover, primarily based on the panoramic radiography findings, the prognosis of tooth No. 14 was hopeless (Determine 6A); due to this fact, extraction of tooth No. 14 and flap surgical procedure for implant No. 12 have been deliberate. An intrasulcular incision was constructed from the mesial line angle of tooth No. 10 to the distal side of implant No. 12 utilizing #15T and #12 blades. After flap elevation, subgingival calculus and bone loss have been confirmed round tooth No. 11 and implant No. 12, respectively (Determine 6B).
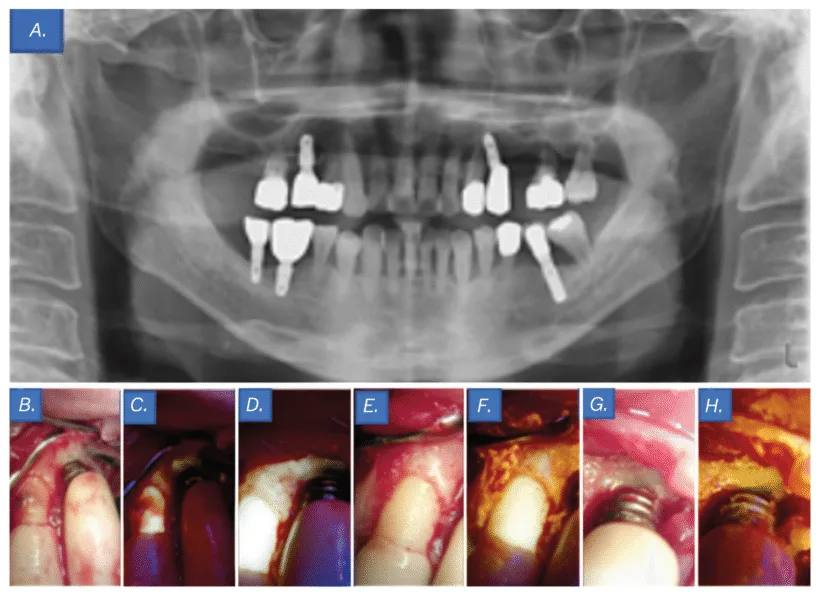
Though no biofilm was seen to the bare eye on the implant No. 12 threads, QLF imaging revealed its presence (Determine 6C). Biofilm elimination was carried out utilizing an ultrasonic scaler (Megagen, Seoul, South Korea), curette, and microbrush. Comply with-up QLF imaging was performed to judge the pre- and post-treatment distinction, confirming profitable biofilm elimination (Determine 6D). The realm was irrigated with tetracycline, and extra medical pictures and QLF photographs have been taken to confirm the elimination of biofilm and an infection at tooth No. 11 and implant No. 12 (Figures 6E-6H). Interrupted sutures have been positioned utilizing 4-0 absorbable artificial sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, USA). The significance of oral hygiene administration was emphasised utilizing visible aids, and tooth brushing instruction (TBI) was offered.
One week after the flap surgical procedure and implant floor decontamination, the affected person returned for suture elimination and reported vital reduction from discomfort. Therapeutic was uneventful, with no notable issues.
On the 6-month follow-up go to, the affected person’s medical signs had resolved. By way of common TBI, implant floor hygiene had improved in comparison with the pre-treatment situation, and the general oral well being remained secure.
Comply with-up abstract (Instances 1–4)
On the 1-week and 6-month follow-up after remedy in Instances 1 by means of 4, medical reassessments demonstrated vital enhancements in gingival irritation, bleeding on probing, and pus discharge. Radiographic examinations confirmed that peri-implant situations remained secure.
This case sequence highlights the potential of BIS expertise within the medical administration of peri-implantitis. Its non-invasive nature and absence of antagonistic results additional assist its worth as a exact and patient-friendly diagnostic and therapeutic adjunct in implant dentistry.
Dialogue
On this case sequence, QLF was used as a supplementary diagnostic instrument for real-time visualization of the lesion standing earlier than and after remedy. This enabled clinicians to establish residual biofilms following the preliminary debridement, permitting for extra thorough implant-surface cleansing.
The usage of the BIS contributed to the event of extra systematic and individualized remedy plans, in the end enhancing the precision and success charge of peri-implantitis administration.
Nevertheless, biofluorescence imaging has some limitations. First, the biofilm we intention to detect is primarily positioned within the apical area quite than within the coronal area. Nevertheless, at present obtainable QLF gadgets have giant heads, making entry to the apical space troublesome. Second, along with the surgeon retracting the cheek and gingiva, an assistant is required to assist in capturing photographs. Moreover, efficient management of bleeding is critical throughout imaging. Third, areas actively exuding pus must be detected as purple on QLF imaging; nonetheless, this was not noticed in few instances. Additional research are required to research this phenomenon. Moreover, research establishing the long-term medical efficacy of peri-implantitis remedy with adjunctive biofluorescence imaging and verifying the effectiveness of biofluorescence imaging by means of comparative research with current diagnostic strategies are required.
Conclusion
This case sequence highlights the usefulness of biofluorescence imaging within the medical administration of peri-implantitis. Biofluorescence imaging is a noninvasive, secure, exact, and patient-friendly diagnostic and therapeutic adjunct in implant dentistry.
Editor’s Be aware: The Lead Creator was liable for the information assortment, performing the information evaluation, and the composition of the summary.